
低温对中国居民健康影响的空间差异性分析
作者简介:王琛智(1992-),男,江苏徐州人,硕士生,主要从事公共健康风险分析,灾害风险分析等方面的研究。E-mail:chenzhiwang@mail.bnu.edu.cn
收稿日期: 2016-06-01
要求修回日期: 2016-07-11
网络出版日期: 2017-03-20
基金资助
国家自然科学基金项目(41571493、41571088)
教育部-国家外国专家局高等学校创新引智计划(B08008)
Analyzing the Spatial Differences of the Relationships Between Low Temperature and Health Risk in China
Received date: 2016-06-01
Request revised date: 2016-07-11
Online published: 2017-03-20
Copyright
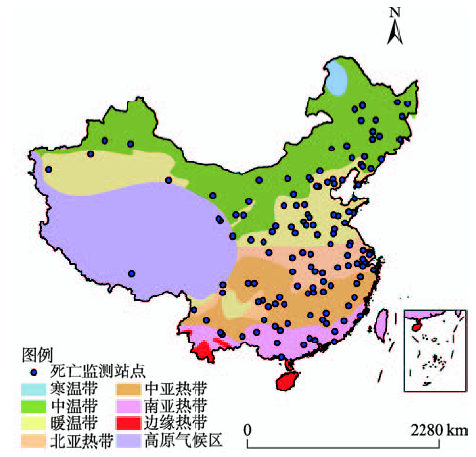
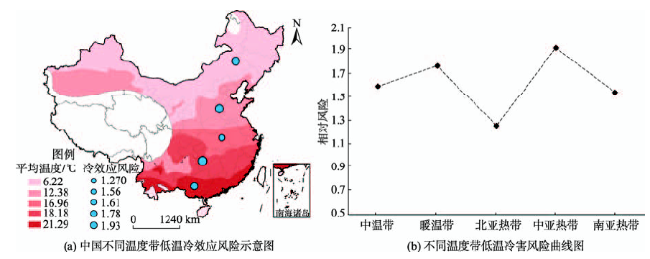
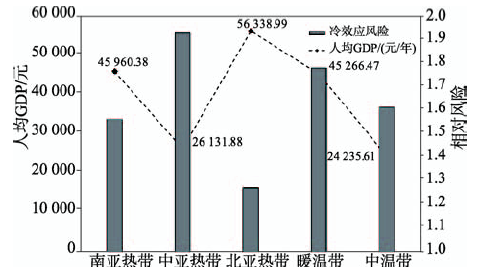
全球变暖导致气象灾害频发,尤其是极端天气事件。极端温度对公共健康的影响已成为当今研究的热点问题之一。相比于发达国家,中国在该领域研究起步较晚。虽然已有出色的成果,但在以下3个方面还略显不足:① 大多数研究基于一个城市或几个城市,缺乏基于大量数据的区域尺度的研究;② 已有研究往往按地理因素或行政单位来划分区域,而忽视区域内部温度的异质性;③ 相比高温热浪,鲜少有研究关注低温冷害的影响。针对上述问题,本文收集了中国疾病预防控制中心2007-2012年全国127个站点的数据,利用分布式滞后非线性模型,探究了中国5个温度带温度与居民非意外死亡之间的暴露-反应曲线。在此基础上,定义当地温度分布1%处的温度为极端低温,根据温度-死亡风险曲线,计算了冷害造成的死亡风险。结果表明,不同温度带的温度-死亡关系曲线呈现U型或J型。极端低温对北亚热带影响最小,其相对风险为1.27(95%CI: 0.94-1.72);对中亚热带影响最大,其相对风险为1.93(95%CI: 1.08-3.60)。随着温度带温度的升高,低温冷效应的影响呈现“M”型,这一特征与不同温度带经济发展有关。因此,不同地区的政府除了应着力提高地区经济发展外,还应根据地区特征,采取更积极有效的措施来应对低温冷害可能给当地公共健康造成的威胁。
王琛智 , 张朝 , 周脉耕 , 殷鹏 , 陶福禄 , 金月雄 . 低温对中国居民健康影响的空间差异性分析[J]. 地球信息科学学报, 2017 , 19(3) : 336 -345 . DOI: 10.3724/SP.J.1047.2017.00336
Global warming has increased the frequency of meteorological disasters, especially extreme temperature events. Many previous studies have reported that human health risk is very sensitive to temperature and climate change was considered to be the most severe global health threat in the 21st century. Nowadays, the research on the impact of extreme temperature on public health has been a hotspot. Compared to those in developed countries, the related studies have started late in China. Moreover, there are three limitations in these studies. (1) Most of such studies focused only on one city or a few cities and the studies on the whole country are few.(2) The previous studies have not quantitatively identified the influence of temperature on health because the spatial scales were based on administrative regions, not on temperature zones. (3) Comparing with many studies on hot wave, relatively fewer are concerned with the influence of extreme low temperature. To overcome aforementioned problems, we collected the mortality dataset and meteorological variables of 127 communities in China during 2007 to 2012 from China Center for Disease Control and Prevention and pooled the community-specific cold risk in various latitude-effected temperature zones with the meta-analysis method. Then, we utilized the Distributed lag non-linear model (DLNM) at community level to investigate temperature-mortality relationship in different temperature zones and calculated the relative risk (RR) of extreme low temperature on mortality. The results showed that although temperature-mortality curves at the community level appeared huge differences, the pooled curves were generally U- or J- shaped in these five zones. Temperature-mortality curves in three zones (the sub-temperate region, warm temperate region and north subtropical region) were all U-shaped, indicating both low and high temperatures could increase significantly mortality risk. Moreover, the curves appeared J-shaped in other two zones (the middle subtropical region and south subtropical region). The most significant cold effect was observed in middle subtropical, with a RR of 1.93 (95% CI: 1.08-3.60); while the cold effect in north subtropical was not so obvious, with a RR of 1.27 (95% CI: 0.94-1.72). Based on this, an M-shaped curve of the cold risk was found across Chinese mainland. This means the risks of cold-related mortality are high in warm temperature and middle subtropical zone, moderate in sub-temperate and south subtropical zone, and low in north subtropical zone. Low temperature does show significant impact on temperature-mortality risk, but considering the M-shaped risk curve, we believe social-economic factors should also be taken into consideration. To explain this phenomenon, we collected the social-economic data including population and GDP and found that the highest per capita GDP matched with the lowest cold-related risk, while the related lower per capita GDP matched with the highest cold-related risk. Based on these findings, different characteristics of mortality of cold stress highlighted that not only ambient temperature but also social-economic condition can be a main factor controlling health risk. Our findings also suggest that more adaptive and effective measures especially increasing investment on public health are necessary, especially for the middle subtropical zone, to reduce health risks in China.
Fig. 1 The distribution map of 127 DSPs covered in this study图1 本研究所用死亡监测站点空间分布示意图 |
Tab. 1 Summary statistics for five temperature zones from 2007 to 2012表1 各区域2007-2012年气象因素、居民死亡情况和经济因素基本情况 |
| 中温带 | 暖温带 | 北亚热带 | 中亚热带 | 南亚热带 | |
|---|---|---|---|---|---|
| 死亡监测站数目 (城市,农村) | 26 (12, 14) | 35 (14,21) | 28 (12, 16) | 19 (6, 13) | 14 (5, 9) |
| 日均非意外死亡数目 | 6(0, 65) | 9(0,78) | 8(0, 142) | 7(0, 67) | 9(0, 58) |
| 气温均值/°C (最小值,最大值) | 6.22 (-0.50, 33.08) | 12.38 (-8.36, 32.80) | 16.96 (-5.76, 33.89) | 18.18 (-5.41, 34.15) | 21.29 (0.21, 32.25) |
| 相对湿度均值/% | 58.69 | 62.47 | 72.92 | 74.73 | 74.87 |
| 人均GDP/元 | 24235.61 | 45266.47 | 56338.99 | 26131.88 | 45960.38 |
| 人口/万人 | 1521.48 | 1995.26 | 1488.86 | 996.54 | 875.07 |
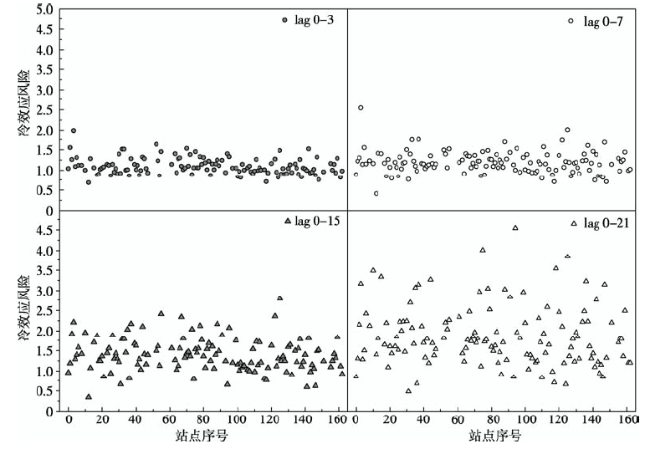
Fig. 2 Relationship between different lag days and model results图2 不同滞后时间与模型结果的关系 |
Tab. 2 List of temperature-mortality curves at community level in different temperature zones表2 不同温度带站点尺度温度-死亡曲线列举 |
 |
Fig. 3 Relationships between low temperature and mortality risk across different temperature zones of China图3 中国不同温度带低温与死亡风险关系 |
Tab. 3 A comparison of the risk calculated by Geodetector and Meta analysis表3 地理探测器计算低温风险与Meta分析结果对比 |
| 分层变量 | 中温带 | 暖温带 | 北亚热带 | 中亚热带 | 南亚热带 |
|---|---|---|---|---|---|
| 地理探测器分析结果 | 1.69 | 1.81 | 1.20 | 1.92 | 1.64 |
| Meta分析风险结果 | 1.61 | 1.78 | 1.27 | 1.93 | 1.56 |
Tab. 4 Significant difference of cold effect among different temperature zones表4 不同温度带冷效应风险显著性差异 |
| Sig. t test:0.05 | 中温带 | 暖温带 | 北亚热带 | 中亚热带 | 南亚热带 |
|---|---|---|---|---|---|
| 中温带 | |||||
| 暖温带 | N | ||||
| 北亚热带 | Y | Y | |||
| 中亚热带 | N | N | Y | ||
| 南亚热带 | N | N | Y | N |
Fig. 4 Cold-effect risk in different temperature zones and their situation of GDP per capita图4 不同温度带冷效应风险和人均GDP情况 |
The authors have declared that no competing interests exist.
| [1] |
WHO. The World Health Report 2008 - primary Health Care(Now More Than Ever)[Z]. 2010.
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
[
|
| [16] |
[
|
| [17] |
[
|
| [18] |
[
|
| [19] |
[
|
| [20] |
|
| [21] |
[
|
| [22] |
[
|
| [23] |
[
|
| [24] |
|
| [25] |
[
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
[
|
| [37] |
[
|
| [38] |
[
|
| [39] |
|
| [40] |
|
| [41] |
|
| [42] |
|
| [43] |
|
| [44] |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}