
Journal of Geo-information Science >
Exploration on Geospatial Risk Assessment in China based on Multiple Data: A Case Study of COVID-19 Data from January 1 to April 11, 2020
Received date: 2020-05-31
Revised date: 2020-08-22
Online published: 2021-04-25
Supported by
Natural Science Foundation of Anhui Province(2008085ME160)
Copyright
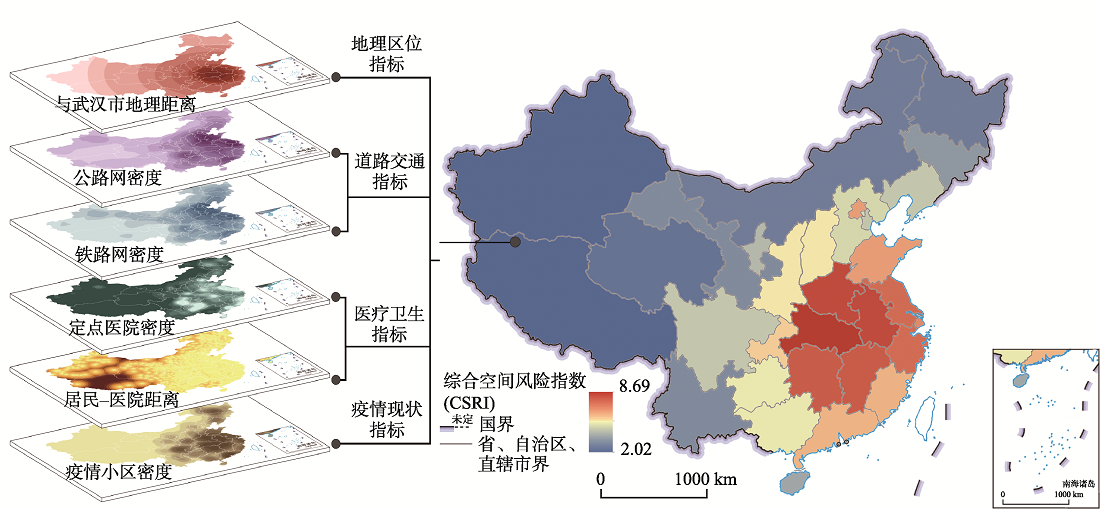
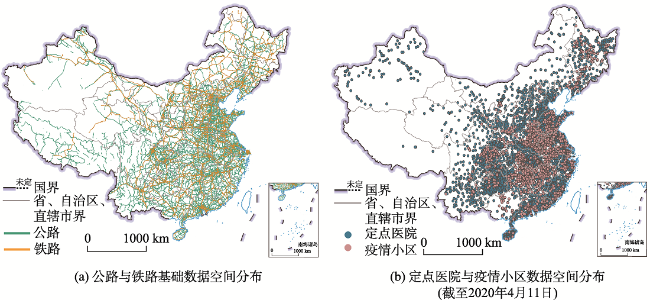
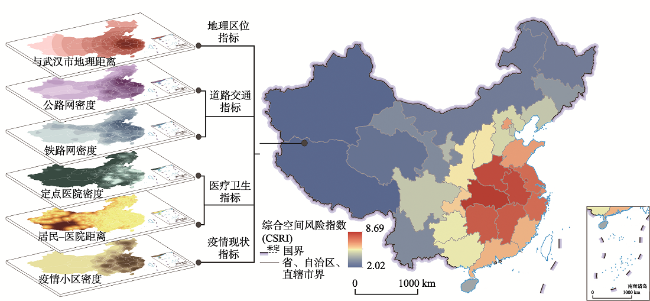
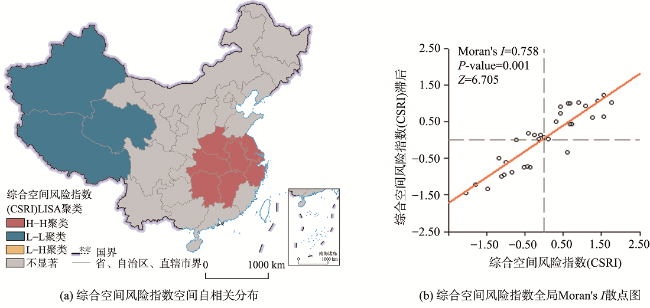
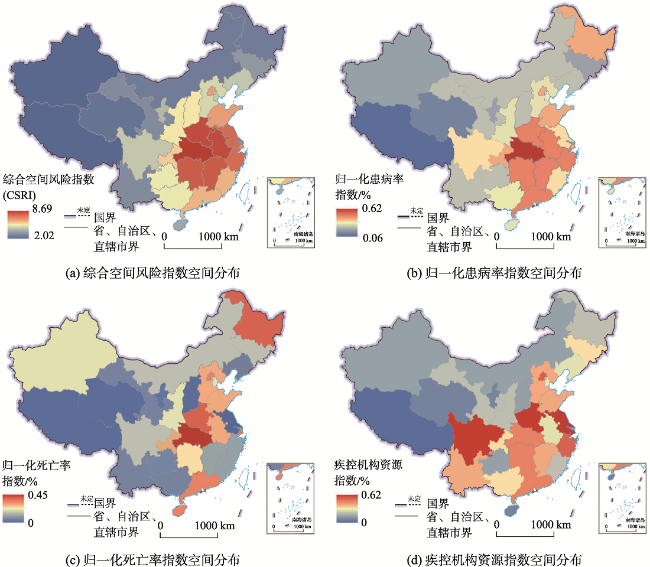
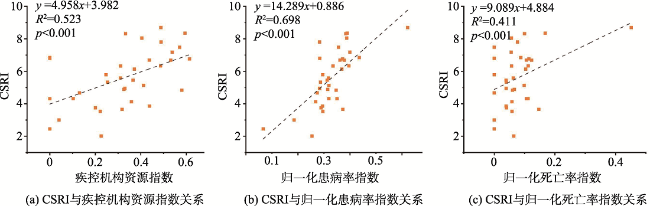
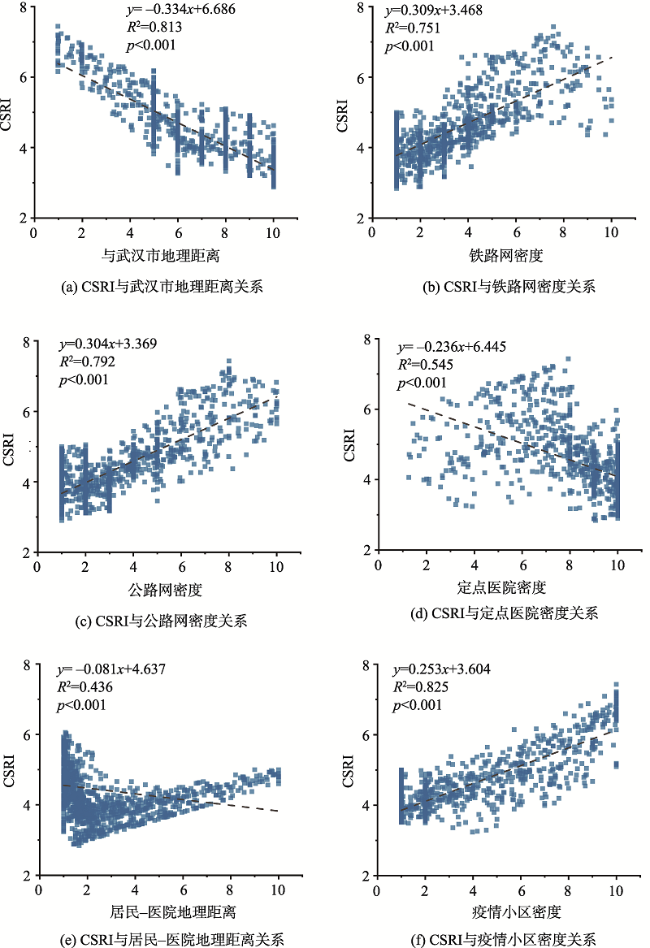
COVID-19 has a spatial transmission risk and poses a threat to the safety and health of the city. Preventing the spread of COVID-19 is therefore the urgent need for society now. The COVID-19 experienced a process that occurred, developed rapidly and stabilized from January 1 to April 11, 2020. Using the initial COVID-19 data for macro-level epidemic risk assessment can provide a certain reference for epidemic prevention and control measures. In this study, by using multiple data, including administrative division data, designated hospital data, epidemic community data, and road traffic data, we proposed a macro-level geospatial risk assessment and validated its effectiveness in China. Based on this, this study also analyzed the construction factors of geospatial risk assessment in order to explore its distribution rules. The following four conclusions showed that: ① Geospatial risk assessment of Covid-19 in China is effective to some extent. ② The spatial distribution of global Moran's I index of geospatial risk in China was 0.758, which had significant spatial agglomeration characteristics. At the same time, the LISA index in different provinces showed spatial differences. Some regions, including Hubei, Henan, Hunan, Jiangxi, Anhui, Zhejiang, Jiangsu, and Shanghai, were identified as high-high clusters and accounted for 25.81% of the provinces in China. The geospatial risk of these provinces was higher. Regions like Qinghai, Tibet, and Xinjiang, with a low degree of geospatial risk, accounted for 9.68% of the provinces in the country. ③ Some indicators, including geographic location indicators, road traffic indicators, medical and health indicators, and epidemic status indicators, were related to the distribution of geospatial risk. According to the statistical Pearson correlation analysis, there were differences in the correlation index R 2. In terms of numerical values, the epidemic status indicators, geographic location indicators, road traffic indicators, and medical and health indicators were ranked from highest to lowest. Different secondary factors were composed of four indicators, and they exhibited two effects of positive and negative correlation. Specifically, the factor of geographic distance from Wuhan, the designated hospital density factor, and the resident-hospital geographical distance factor showed significant negative correlations, with R 2 of 0.813, 0.545, and 0.436, respectively. However, the remaining factors showed significant positive correlations, including railway network density factor, road network density factor, and epidemic community density factor, and their R 2 were 0.751, 0.792, and 0.825, respectively. ④ The components of geospatial risk were intricate and complicated by multiple factors. According to the spatial stratified heterogeneity analysis, we found that there were interactions between different factors. Among them, the resident-hospital geographic distance factor interacted strongly with the railway network density factor and the road network density factor, and their q values were 0.9842 and 0.9837, respectively. This study not only explored the spatial resource allocation of major epidemics in urban management, but also provided a basis for regional spatial prevention and control strategies.
FANG Yunhao , GU Kangkang . Exploration on Geospatial Risk Assessment in China based on Multiple Data: A Case Study of COVID-19 Data from January 1 to April 11, 2020[J]. Journal of Geo-information Science, 2021 , 23(2) : 284 -296 . DOI: 10.12082/dqxxkx.2021.200273
表1 中国综合空间风险评估因子及其权重Tab. 1 Comprehensive spatial risk assessment factors and their weights in China |
| 评估因子 | 地理区位 | 道路交通 | 医疗卫生 | 疫情现状 | ||
|---|---|---|---|---|---|---|
| 与武汉市地理距离 | 公路网密度 | 地铁网密度 | 定点医院密度 | 居民-医院地理距离 | 疫情小区密度 | |
| 权重 | 0.250 | 0.125 | 0.125 | 0.125 | 0.125 | 0.250 |
表2 中国疾控机构资源指标及其权重Tab. 2 Disease control agency resource indicators and their weights in China |
| 指标 | 达标情况 | 平均使用面积 | 机构数 | 总编制人数 | 使用仪器情况 |
|---|---|---|---|---|---|
| 属性 | + | + | + | + | + |
| 权重 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 |
注:表中“+”表示其指标与全国疾控机构资源呈正相关。 |
表3 2020年1月1日至4月11日中国综合空间风险指数(CSRI)与各变量对比统计Tab. 3 Comparative statistics of Comprehensive Spatial Risk Index (CSRI) and various variables in China from January 1 to April 11, 2020 |
| 地区 | CSRI | 排名 | 疾控机构资源指数 | 残差 | 归一化患病率指数 | 残差 | 归一化死亡率指数 | 残差 |
|---|---|---|---|---|---|---|---|---|
| 湖北 | 8.69 | 1 | 0.49 | -6 | 0.62 | 0 | 0.45 | 0 |
| 河南 | 8.35 | 2 | 0.59 | 0 | 0.39 | -2 | 0.17 | 0 |
| 安徽 | 8.32 | 3 | 0.33 | -14 | 0.38 | -4 | 0.10 | -6 |
| 江西 | 8.05 | 4 | 0.40 | -9 | 0.39 | -3 | 0.06 | -11 |
| 湖南 | 7.81 | 5 | 0.49 | -3 | 0.28 | -20 | 0.08 | -7 |
| 江苏 | 7.48 | 6 | 0.57 | +2 | 0.36 | -5 | 0.00 | -21 |
| 浙江 | 7.18 | 7 | 0.54 | +2 | 0.40 | +5 | 0.06 | -7 |
| 上海 | 6.76 | 8 | 0.61 | +7 | 0.37 | 0 | 0.11 | +2 |
| 山东 | 6.68 | 9 | 0.44 | -1 | 0.36 | -3 | 0.11 | +2 |
| 北京 | 6.68 | 10 | 0.53 | +4 | 0.38 | +4 | 0.12 | +6 |
| 广东 | 6.33 | 11 | 0.49 | +2 | 0.40 | +8 | 0.11 | +6 |
| 福建 | 6.33 | 12 | 0.31 | -9 | 0.33 | -2 | 0.06 | -5 |
| 重庆 | 6.13 | 13 | 0.37 | -1 | 0.37 | +4 | 0.10 | +3 |
| 山西 | 5.79 | 14 | 0.25 | -9 | 0.30 | -6 | 0.00 | -14 |
| 陕西 | 5.58 | 15 | 0.31 | -7 | 0.32 | -1 | 0.06 | -3 |
| 广西 | 5.45 | 16 | 0.37 | +1 | 0.31 | -2 | 0.04 | -6 |
| 贵州 | 5.33 | 17 | 0.25 | -7 | 0.29 | -6 | 0.04 | -7 |
| 河北 | 5.14 | 18 | 0.41 | +6 | 0.32 | +3 | 0.10 | +7 |
| 辽宁 | 4.95 | 19 | 0.33 | +1 | 0.28 | -7 | 0.04 | -7 |
| 天津 | 4.89 | 20 | 0.33 | +1 | 0.31 | +1 | 0.07 | +7 |
| 四川 | 4.83 | 21 | 0.58 | +18 | 0.35 | +8 | 0.06 | +5 |
| 宁夏 | 4.67 | 22 | 0.13 | -6 | 0.27 | -6 | 0.00 | -7 |
| 海南 | 4.32 | 23 | 0.10 | -6 | 0.32 | +6 | 0.11 | +15 |
| 吉林 | 4.13 | 24 | 0.36 | +8 | 0.27 | -3 | 0.06 | +4 |
| 云南 | 3.86 | 25 | 0.44 | +14 | 0.29 | +3 | 0.04 | +2 |
| 甘肃 | 3.75 | 26 | 0.20 | -1 | 0.29 | +2 | 0.04 | +1 |
| 黑龙江 | 3.66 | 27 | 0.32 | +7 | 0.37 | +17 | 0.15 | +24 |
| 内蒙古 | 3.53 | 28 | 0.22 | 2 | 0.30 | +7 | 0.06 | +9 |
| 青海 | 3.00 | 29 | 0.04 | -1 | 0.19 | -1 | 0.00 | -1 |
| 西藏 | 2.45 | 30 | 0.00 | -1 | 0.07 | -1 | 0.00 | -1 |
| 新疆 | 2.02 | 31 | 0.23 | 6 | 0.25 | +2 | 0.06 | +10 |
注:残差表示与CSRI指数排名差异;各变量指数均经过归一化处理,非真实数字;由于数据获取困难,本研究不包括港香港、台湾和澳门。 |
表4 2020年1月1日至4月11日中国地理空间疫情风险评估因子探测结果Tab. 4 Detection results of geospatial epidemic risk factors in China from January 1 to April 11, 2020 |
| 因子 | 与武汉市地理距离 | 铁路网密度 | 公路网密度 | 定点医院密度 | 居民-医院地理距离 | 疫情小区密度 |
|---|---|---|---|---|---|---|
| q 统计值 | 0.8355 | 0.8103 | 0.8214 | 0.7649 | 0.6053 | 0.8139 |
| p 值 | 0.0000 | 0.0215 | 0.0343 | 0.0000 | 0.0127 | 0.0000 |
注:p<0.05具有统计意义。 |
表5 2020年1月1日至4月11日中国地理空间疫情风险评估因子交互作用结果Tab. 5 Interaction results of geospatial epidemic risk factors in China from January 1 to April 11, 2020 |
| 因子 | 与武汉市地理距离 | 铁路网密度 | 公路网密度 | 定点医院密度 | 居民-医院地理距离 | 疫情小区密度 |
|---|---|---|---|---|---|---|
| 与武汉市地理距离 | 0.8355 | |||||
| 铁路网密度 | 0.9252(Y) | 0.8103 | ||||
| 公路网密度 | 0.9309(Y) | 0.9034(N) | 0.8214 | |||
| 定点医院密度 | 0.9210(Y) | 0.8934(Y) | 0.8957(Y) | 0.7649 | ||
| 居民-医院地理距离 | 0.9687(Y) | 0.9837(Y) | 0.9842(Y) | 0.9781(Y) | 0.6053 | |
| 疫情小区密度 | 0.9102(Y) | 0.8834(N) | 0.8908(N) | 0.8755(Y) | 0.9803(Y) | 0.8139 |
注:Y代表有显著性差异,N代表没有显著性差异。 |
| [1] |
|
| [2] |
|
| [3] |
朱斌, 刘锦林, 毛瑛. 中国典型法定报告传染病发病率空间关联性分析[J]. 中国公共卫生, 2018,34(1):4-8.
[
|
| [4] |
丁晓彤, 余卓渊, 宋海慧, 等. 基于信息熵的中国自然疫源性疾病分布特征研究[J]. 地球信息科学学报, 2019,21(12):1877-1887.
[
|
| [5] |
高芳旭, 齐秀英. 天津市和平区细菌性痢疾流行特征及疫情预测[J]. 现代预防医学, 2015,42(11):1951-1953.
[
|
| [6] |
陈会宴, 廖一兰, 张宁旭, 等. 山西省原平市神经管畸形时空分析[J]. 地球信息科学学报, 2017,19(4):502-510.
[
|
| [7] |
张湘雪, 王丽, 尹礼唱, 等. 京津唐地区HFMD时空变异分析与影响因子探测[J]. 地球信息科学学报, 2019,21(3):398-406.
[
|
| [8] |
|
| [9] |
叶莹, 范威, 王海峰, 等. 河南省新型冠状病毒肺炎聚集性疫情流行病学特征分析[J]. 中国公共卫生, 2020,36(4):465-468.
[
|
| [10] |
|
| [11] |
唐燕. 新冠肺炎疫情防控中的社区治理挑战应对:基于城乡规划与公共卫生视角[J]. 南京社会科学, 2020(3):8-14,27.
[
|
| [12] |
杨俊宴, 史北祥, 史宜, 等. 高密度城市的多尺度空间防疫体系建构思考[J]. 城市规划, 2020,44(3):17-24.
[
|
| [13] |
中华人民共和国国家卫生健康委员会. 截至4月11日24时新型冠状病毒肺炎疫情最新情况[EB/OL]. http://www.nhc.gov.cn/,2020-04-12.
[ National Health Commission, PRC. COVID-19 update as of 11 April 24:00[EB/OL]. http://www.nhc.gov.cn/,2020-04-12.]
|
| [14] |
National data[DB/OL]. http://data.stats.gov.cn/search.htm?s/.
|
| [15] |
The Data-center of China Public Health Science[DB/OL]. http://www.phsciencedata.cn/Share/en/index.jsp.
|
| [16] |
Openstreetmap[DB/OL]. http://download.geofabrik.de/.
|
| [17] |
China Data Lab Dataverse[DB/OL]. https://dataverse.harvard.edu/.
|
| [18] |
刘耀宝, 曹俊. 我国境外输入性疟疾防控策略对当前新型冠状病毒肺炎防控工作的启示[J]. 中国血吸虫病防治杂志, 2020,32(2):113-118.
[
|
| [19] |
|
| [20] |
许小可, 文成, 张光耀, 等. 新冠肺炎爆发前期武汉外流人口的地理去向分布及影响[J]. 电子科技大学学报, 2020,49(3):324-329.
[
|
| [21] |
张宇, 田万利, 吴忠广, 等. 基于改进SEIR模型的新冠肺炎疫情沿交通线路传播机制[J]. 交通运输工程学报, 2020,20(3):150-158.
[
|
| [22] |
李欣, 周林, 贾涛, 等. 城市因素对COVID-19疫情的影响——以武汉市为例[J]. 武汉大学学报·信息科学版, 2020,45(6):826-835.
[
|
| [23] |
|
| [24] |
李刚, 李建平, 孙晓蕾, 等. 主客观权重的组合方式及其合理性研究[J]. 管理评论, 2017,29(12):17-26,61.
[
|
| [25] |
郑斓, 任红艳, 施润和, 等. 珠江三角洲地区登革热流行风险空间模拟与预测[J]. 地球信息科学学报, 2019,21(3):407-416.
[
|
| [26] |
张永树, 杨振凯, 訾璐, 等. 中国艾滋病空间格局和时空演化分析[J]. 地球信息科学学报, 2020,22(2):198-206.
[
|
| [27] |
张新, 林晖, 朱长明, 等. COVID-19疫情早期中国确诊时间的时空特征及动态过程分析[J]. 武汉大学学报·信息科学版, 2020,45(6):791-797.
[
|
| [28] |
|
| [29] |
张婷, 程昌秀. 顾及空间集聚程度的中国高温灾害危险性评价[J]. 地球信息科学学报, 2019,21(6):865-874.
[
|
| [30] |
陈芳, 吴家兵, 姜静静, 等. 安徽省新型冠状病毒肺炎聚集性疫情流行特征与防控措施分析[J]. 中国公共卫生, 2020,36(4):469-472.
[
|
| [31] |
刘勇, 杨东阳, 董冠鹏, 等. 河南省新冠肺炎疫情时空扩散特征与人口流动风险评估——基于1243例病例报告的分析[J]. 经济地理, 2020,40(3):24-32.
[
|
| [32] |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}